
Therapy is one of the fastest ways a home health chart can go from “looks fine” to “why did we get denied?”
One clinician documents “gait training provided” and thinks that’s enough. Another writes “maintenance program taught” but never shows why a therapist had to do it. Then an ADR hits, or a payer asks for records, and suddenly leadership is stuck trying to answer a question that feels deceptively simple:
“Was this therapy actually skilled under Medicare, and did we prove it?”
*This article was written in consultation with Mariam Treystman.
At The Home Health Consultant (THHC), we help Medicare-certified agencies build compliance systems that hold up under review & increasing regulatory scrutiny.
We’re writing this article to give you a beginner-friendly, Medicare-aligned way to understand how the rules get applied differently to PT, SLP, and OT. After reading, you’ll have a more clear understanding of the differences, so you can communicate better with industry professionals and agency staff (and support your clinicians without turning them into billing experts).
Disclaimer: This article is for educational purposes only. The Home Health Consultant (THHC) is not providing clinical, billing, or legal advice. Therapy coverage decisions must be based on individualized clinical judgment and current Medicare regulations. Always consult your qualified clinicians, billing specialists, and the official Medicare guidelines when making coverage determinations.
What Medicare Coverage Rules Apply to All Three Therapy Disciplines in Home Health?
Physical Therapy (PT), Speech Language Pathology (SLP), and Occupational Therapy (OT) treat different problems. But, Medicare applies a shared baseline expectation to all: therapy must be reasonable and necessary and must require therapist-level skill based on the patient’s clinical situation.
Medicare does not grant coverage just because a plan of care says “restorative therapy” or “maintenance therapy.” Instead, Medicare focuses on what the record shows at the visit level:
- Why the patient needed skilled involvement that day
- Whether the plan is supported by objective functional measurement
- Whether documentation shows response and next steps
This article focuses on how those expectations look when applied within each discipline.

What Are Medicare’s “Defined Points,” and Why Do They Matter in Home Health Therapy Coverage?
Medicare requires that therapy be formally measured at specific times during treatment. Those measurements must be completed by a qualified therapist, not an assistant.
In practical terms, this means two things for each discipline providing therapy:
1. At the Initial Therapy Visit
A qualified therapist must:
- Personally complete the visit (an assistant cannot)
- Assess the patient’s function using objective measurement
- Document findings in a way that allows comparison over time
Medicare gives examples of functional areas across disciplines that may be measured, including but not limited to:
- Walking and stair climbing
- Bathing, dressing, and toileting
- Swallowing (for SLP)
- Use of assistive devices
- Cognitive or mental factors
2. At Least Every 30 Days After That (Per Discipline)
For each therapy discipline:
- A qualified therapist must personally complete the ordered visit
- The therapist must reassess function
- The therapist must compare the new findings to prior measurements
- The therapist must document whether therapy is effective (or explain why skilled care is still needed)
In short: Medicare isn’t just asking whether therapy is being provided. Medicare wants to know whether therapist-level involvement and measurable functional reassessment are occurring at required intervals. They do so by making sure your records clearly show it.
How Does the 30-Day Reassessment Clock Work When Multiple Disciplines Are Involved?
When multiple therapy disciplines are involved, Medicare requires each discipline to follow its own separate 30-day reassessment clock. These clocks do not overlap or reset each other.
This is one of the easiest rules to misunderstand, so here’s the simplest way to frame it:
- The 30-day clock is discipline-specific
- It begins with the first therapy service for that discipline
- It resets each time the therapist (not the assistant) completes the reassessment visit with objective measurement and documentation
So if PT starts first and OT starts later, they do not share a single 30-day timer. Each discipline has its own.
What Does Medicare Mean by “Objective Functional Measurement” in Everyday Documentation?
Think of ‘objective functional measurements’ as “showing your work.”
Medicare is not asking for fancy language. Medicare is asking for documentation that allows a reviewer to see:
- What function looked like at baseline
- What function looks like now
- What changed (or why skilled involvement remains necessary)
- What the therapist plans to do next based on the findings
Medicare does not name one required standardized test (for example, it doesn’t say “you must use Test X, Y, or Z”). So, Medicare isn’t dictating the exact tool. It’s dictating the standard the measurement must meet.
Long story short, Medicare wants to see how the service has progressed over time in specific, measurable terms. For example, walking needs to be shown in feet at start, and at each point. If improvements aren’t made, then the care plan is adjusted. The service isn’t justifiable if it’s not producing a positive result over time.
How Can Agencies Quickly Remember What Medicare Is Looking for in PT vs SLP vs OT?
Here’s a simple visual aid you can use in training or chart review. It’s not a billing table, instead it’s a very general “coverage focus” guide.
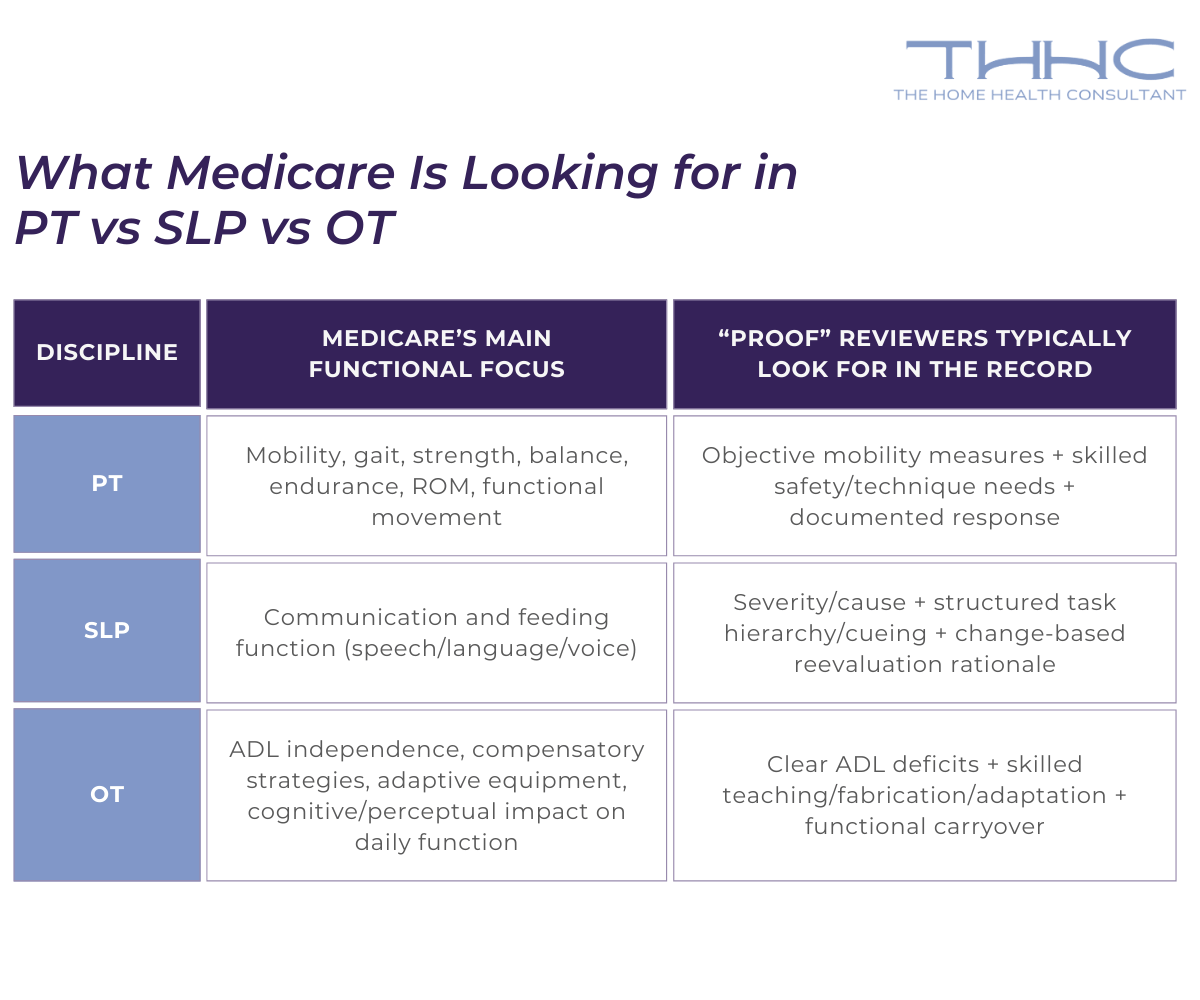
Keep in mind: Medicare still expects the same backbone for all three disciplines:
- Skilled need
- Reasonable/necessary care
- Defined-point measurement
- Documentation that tells the story
Now let’s dive deeper into each individual discipline.
How Does Medicare Apply These Rules to Physical Therapy in Home Health?
Medicare recognizes PT assessment and periodic reassessment as skilled when the therapist is evaluating rehab needs and potential, or developing/implementing a PT program.
In practice, Medicare identifies objective tests and measurements such as:
- Range of motion
- Strength
- Balance
- Coordination
- Endurance
- Functional ability
Example scenario (PT assessment):
A patient’s walking has been impaired by scar tissue from burns. PT evaluates gait, establishes a gait training plan, and documents objective functional findings and the patient’s response. Medicare expects those measurements to be compared again at defined points so effectiveness can be determined.
How Does Medicare Apply These Rules to Speech-Language Pathology in Home Health?
Medicare covers SLP when the patient’s clinical condition requires the specialized judgment, knowledge, and skills of a qualified SLP.
SLP services may be covered when directed toward:
- Speech/voice production
- Communication function
- Feeding activities
Medicare also states SLP may be covered when services are reasonably expected to improve, maintain, or prevent/slow deterioration in communication or feeding.
When Is an SLP Reevaluation Reasonable and Necessary Under Medicare?
Medicare doesn’t treat reevaluations as automatic. Reevaluation is reasonable and necessary only if the patient has:
- A change in functional speech or motivation
- Clearing of confusion
- Remission of another condition that previously contraindicated SLP
Also important: during restorative SLP, routine reevaluations are considered part of therapy and are not separately billable.
How Does Medicare Apply These Rules to Occupational Therapy in Home Health?

Medicare covers skilled OT when the individualized assessment shows the patient needs OT-level judgment and skill. This is often tied to daily function, safety, compensatory techniques, and adaptive equipment.
Medicare gives concrete examples of OT programs that may be covered when reasonable and necessary, including but not limited to:
- Task-oriented activities to restore physical function (Reaching to brush hair after a shoulder fracture)
- Sensory-integrative work after stroke (Practicing bilateral hand use to stabilize a plate while cutting soft food)
- Psychiatric illness activity programs as part of active treatment (Step-by-step cueing to sequence brushing teeth after a stroke)
- Compensatory techniques for ADLs (Adaptive techniques for safe lower-body dressing after hip fracture)
- Orthotic and self-help devices (utensil device; hand splint for rheumatoid arthritis)
- Vocational/prevocational assessment only when directed toward ADL restoration (not job-specific training)
To sum it up, Medicare separates ADLs (Activities of Daily Living) into two categories:
- Basic ADLs: bathing, dressing, toileting, grooming, eating, transferring, ambulation
- IADLs (Instrumental Activities of Daily Living): cooking, shopping, laundry, housekeeping, medication management
In Medicare home health:
- Therapy services are generally justified when they address basic self-care deficits (Basic ADLs)
- Therapy services are majorly non-covered in Medicare home health when they address IADLs, unless they’re directly tied to improving or compensating for basic ADL safety or independence
How Can Agencies Use These Discipline-Specific Rules to Reduce Therapy Claim Denials?
A simple way to apply this across PT, SLP, and OT is to build your internal review lens around three questions:
- Why did this patient require therapist-level skill for safety or effectiveness today?
- Did the discipline meet the defined-point measurement requirement (initial and at least every 30 days)?
- Do the notes show objective findings, response, and next steps — not just that a visit occurred?
When the answer is clearly supported in the record, therapy decisions become much easier to defend across all disciplines.
Want to Pressure-Test Your Therapy Documentation Before Medicare Does?
Everything we just discussed must be clearly supported in the clinical record. If it’s not documented correctly, it doesn’t ‘count’.
Your next step is learning how to check your own charts to confirm you’re actually meeting those standards.
Check out our article on Best Practices for Conducting Chart Audits to learn how to structure chart audits and identify documentation risks before a surveyor or auditor does.

*Disclaimer: The content provided in this article is not intended to be, nor should it be construed as, legal, financial, or professional advice. No consultant-client relationship is established by engaging with this content. You should seek the advice of a qualified attorney, financial advisor, or other professional regarding any legal or business matters. The consultant assumes no liability for any actions taken based on the information provided.
Topics:

















.png?width=850&height=400&name=Rando%20(7).png)
{kind=link}